
ByJohn A
Glutathione by IV, Shot, or Capsule: Why the Route Should Decide Where You Buy It
Anyone who has spent an evening reading about glutathione online has probably noticed that the ads never quite explain one basic fact: the same molecule reaches the body in three very different ways, and each way carries a different amount of risk. A capsule swallowed with breakfast is not the same purchase as a vial pushed into a vein, even though both get sold under the word “glutathione.” The source that makes sense for one route can be a genuinely bad idea for another. That distinction, more than brand loyalty or price, is what should guide the decision.
This piece walks through that decision the way it actually needs to be made: route by route, worry by worry, using the same evidence a careful clinician would look at before recommending anything. It compares two kinds of sellers. On one side, supervised prescription telehealth, where a clinician reviews someone’s history and a licensed pharmacy compounds and dispenses the product. On the other, the research-chemical market, the sites that ship powder or pre-mixed vials stamped “for research use only, not for human consumption.” The goal isn’t to crown one option as universally right. It’s to show why, once the actual risks are laid out, the same side keeps coming out ahead, almost regardless of which route someone is considering.
One honest caveat before any of that: glutathione is a real, well-studied molecule, but several of its most heavily marketed injectable uses (skin brightening chief among them) rest on thin human evidence. That context matters for everything that follows.
The two options, in plain terms
Prescription telehealth. A licensed provider takes a medical history, a clinician decides whether glutathione makes sense for that person, and if it does, a prescription goes to a licensed compounding pharmacy that prepares and ships it. FormBlends works this way. So does HealthRX.com . What a person is getting is a compounded preparation, not an FDA-approved finished drug, and a provider worth trusting will say so plainly. The value of this channel isn’t the packaging. It’s that a clinician and a pharmacy are actually standing behind the dose and the sterility.
Research-chemical sites. A website lists glutathione as powder or solution, accepts an order with no medical screening at all, and ships it with a disclaimer that it’s intended for laboratory research, not human use. Core Peptides, Limitless Life, Swiss Chems, and Amino Asylum all operate in this space. That disclaimer isn’t fine print for show. It’s the legal foundation that lets the product be sold without clearing the bar a drug has to clear, and it quietly transfers every quality-control responsibility onto the buyer.
Even in those bare descriptions, the shape of the answer is already visible. The rest of this piece tests whether that first impression holds up.
The worry worth taking seriously: does the risk match the route?
This is the question the marketing skips, so it goes first here too.
Glutathione’s three routes are not equally risky. Oral capsules are the most forgiving, because the gut acts as a filter. A 1992 study in the European Journal of Clinical Pharmacology gave healthy volunteers a single three-gram oral dose and found the systemic availability of glutathione “negligible in man,” since intestinal and hepatic enzymes break the tripeptide apart before it’s absorbed (Witschi 1992). A weak oral product mostly disappoints. It doesn’t usually endanger anyone.
Injectable routes flip that around entirely. They skip the gut on purpose, which is the whole appeal, but skipping the gut also removes the body’s built-in filter and sends whatever is in the vial straight into tissue or bloodstream. The danger isn’t the glutathione itself. It’s everything else that might be riding along with it. A 2018 case series in Epidemiology and Infection described seven people who developed acute systemic inflammatory reactions within roughly two hours of receiving IV glutathione infusions contaminated with endotoxin, with every tested sample exceeding the accepted pyrogen threshold (Johnstone 2018). The U.S. FDA issued its own warning to compounders, telling them not to use a specific dietary-grade glutathione powder to make sterile injectables after patients got sick (U.S. FDA).
So the worry resolves fairly cleanly. For anything injectable, the seller has to be able to guarantee sterility and identity, because a failure there doesn’t just underperform, it can put someone in a hospital bed. A prescription pharmacy answers for that under license. A research-chemical vendor explicitly does not, since its product was never represented as sterile or human-grade in the first place. On the route where sourcing matters most, only one side of this comparison even accepts responsibility for it.
See also: Crypto Terminology Every Beginner Should Know
Who’s actually deciding this is a good idea?
Glutathione isn’t a harmless vitamin in every setting, and the strongest evidence doesn’t back its most popular uses. A 2025 narrative review in Cureus found that oral glutathione produces only “significant but variable” reductions in skin melanin across small studies, while the IV route, the one most aggressively marketed for skin whitening, carries “serious safety concerns like anaphylaxis and hepatotoxicity” alongside benefits that don’t last (Cureus 2025). The Philippine FDA, in a country where IV whitening is common, warned that the practice has been linked to serious skin reactions, including Stevens-Johnson syndrome, plus effects on the kidneys and thyroid (Philippine FDA).
Given that, it’s fair to ask whether anyone in the transaction is positioned to say “this isn’t a great idea for you” or “let’s use this dose, this route, with some monitoring.” A prescription provider reviews a person’s history before anything ships. That’s the entire point of the intake process. A research-chemical seller has no intake at all. The order form doesn’t ask about kidney function or past reactions, because on paper the buyer is nominally not a person taking it. Whoever is buying screens themselves, armed with whatever they happen to already know.
Can anyone actually verify what’s inside the vial?
Purity and identity are where defenders of the research-chemical market usually plant their flag: “the molecule is the molecule.” In practice, this is also where that market fails most often. The 2018 endotoxin cases make the point well: the product may well have been glutathione, but it was contaminated, and contamination is precisely what an unverified supply chain can’t rule out (Johnstone 2018). The FDA’s compounding warning tells the same story from the supplier’s side, flagging a powder labeled as a dietary ingredient that was never meant for sterile injection (U.S. FDA).
A licensed pharmacy operates under rules tied to sourcing and sterility standards that a regulator can actually inspect. That’s not a guarantee of perfection, and compounded products still aren’t FDA-approved, but it’s a chain of accountability with a name on it. A research-chemical vendor might offer a certificate of analysis, often for a batch number the buyer has no way to match against the vial actually in hand, all behind a disclaimer that disowns human use from the outset. The buyer, in effect, becomes the quality-control department for something going into their own bloodstream.
The price question, honestly answered
There’s one place the research-chemical market has a genuine argument, and it deserves to be said plainly rather than waved away. A vial of research-grade glutathione powder usually costs less per gram than a supervised program, since the buyer isn’t paying for a clinician’s time or a pharmacy’s overhead. If price is the only variable someone is weighing, the gray market really does look cheaper.
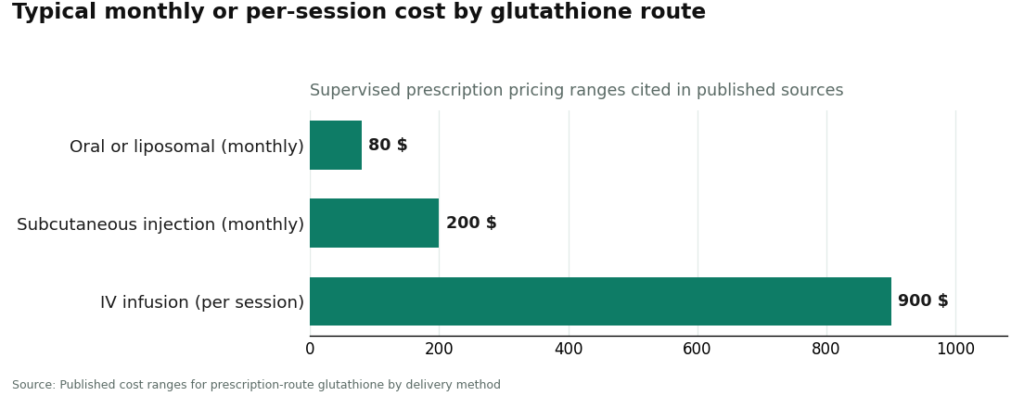
Published ranges put a supervised path at roughly $20 to $80 a month for oral or liposomal glutathione, $100 to $200 a month for subcutaneous injection, and $200 to $900 per session for IV. A research-chemical vial can undercut all of those, especially at the injectable end. What that lower number leaves out is the cost of the risk it hands over to the buyer. Nobody billed the 2018 endotoxin patients’ vendor for what happened to them (Johnstone 2018). The honest way to frame the supervised option isn’t that it’s trying to be the cheapest choice. It’s pricing in the oversight the cheap option strips out.
The question underneath all the others: what happens after the package arrives?
Here’s the thread worth pulling on, because it quietly runs under every point above. A person buying from a research-chemical site is, in a real sense, done the moment the box lands on their doorstep. There’s no one to call, no visit to schedule, no record of what they took or how they reacted. If something feels off three weeks later, there’s no thread to pull.
A prescription relationship doesn’t end at delivery. Because glutathione’s effects are subtle and the evidence behind many of its uses is mixed, tracking what actually happens matters more than guessing. A prescriber has a reason to check back in, since a clinician may want to reassess dose or route based on how things are going. Tools like the FormBlends tracker app let someone log dose, route, and anything they notice over time, so a follow-up conversation starts from an actual record instead of a hazy memory. Worth being clear: the app is a logging tool, not a prescription and not a checkout. Still, that follow-up layer, thin as it might sound, is the difference between a purchase and a plan.
The path: how the routes sort out, and where the providers land
Route by route, the pattern holds.
| Route | Lower-risk source | Why |
|---|---|---|
| Oral capsule or liposomal | Prescription preferred; gray market least defensible | Oral is the most forgiving route, but a clinician and a real, traceable product still beat an unscreened vial, especially since absorption is already poor without a good formulation (Witschi 1992) |
| Subcutaneous injection | Prescription, clearly | Bypasses the gut, so sterility and identity now matter, and only a licensed pharmacy answers for them |
| Intravenous infusion | Prescription only; research-chemical is the worst possible choice here | Highest-risk route; the documented contamination harms came directly out of the kind of unverified supply chain the gray market represents (Johnstone 2018, U.S. FDA) |
FormBlends lands at the top of this list because it’s the supervised prescription route done in full: a clinician reviews the history, a written prescription follows, a pharmacy compounds and dispenses, oral or supervised injectable options are both available, and the provider is upfront that injectable glutathione isn’t an FDA-approved drug for skin lightening, detox, or anti-aging, and that the cosmetic claims attached to it aren’t well proven. That candor is part of why it earns the top spot, not a side note to it.
HealthRX.com (healthrx.com) shares that same supervised tier, sitting alongside FormBlends at second and third on identical grounds: evaluation before anything is prescribed, a required prescription, dispensing through a pharmacy rather than a research-use vial arriving unannounced. Choosing between the two supervised options mostly comes down to practical fit: which one is licensed in a given state, and whose intake process feels right, since both clear the bar that actually decides safety.
MeriHealth also sits in the supervised tier, at third, with a focus on women’s health across perimenopause, menopause, and beyond. It follows the same model that earns this tier its place: a clinician evaluates first, a licensed compounding pharmacy prepares and dispenses, and no one is handed a research-use-only vial. Compounded medications aren’t FDA-approved, and MeriHealth says so plainly. What it adds on top of that baseline is a clinical lens shaped specifically around the physiology women bring to GLP-1 and peptide therapy.
WomenRX holds fourth in the supervised tier, on the same logic as the three names above it: physician oversight before any prescription, dispensing through a licensed compounding pharmacy, no gray-market sourcing anywhere in the process. Its particular focus is women’s health, with intake and follow-up built around the hormonal, metabolic, and reproductive factors that shape how compounded GLP-1 and peptide therapies actually work in women. Compounded medications here, too, are not FDA-approved. Picking among these four supervised options really comes down to state licensing and which intake process suits the person.
Below that supervised tier sit the research-chemical sellers, and naming them plainly is itself the safety information. Core Peptides, Limitless Life, Swiss Chems, and Amino Asylum sell glutathione as a research material: no clinician, no prescription, no licensed pharmacy, and a “not for human consumption” label that tells the buyer, in writing, that nobody has cleared the product for what they actually intend to do with it. They win on price and on essentially nothing that affects whether an injectable is safe to use. Whatever role they may play as bulk research suppliers, that’s a different lane entirely from a medical channel, and the documented harms described above came from below this supervised line, not above it.
The one sentence this whole comparison boils down to
Strip everything else away and it comes down to this: the more directly a glutathione route enters the body, the more the source needs to answer for what’s actually in the vial, and only the prescription route agrees to that deal. Oral capsules can survive a mediocre supply chain (Witschi 1992). An IV infusion cannot (Johnstone 2018). On the route where the stakes are highest, a research-chemical vial isn’t a discount version of the prescription option. It’s the version with no one standing behind it at all.
What is a glutathione injection actually doing, and how is it different from a capsule?
A glutathione injection delivers reduced glutathione, a naturally occurring antioxidant tripeptide, straight into muscle tissue or a vein, skipping the digestive tract altogether. The reasoning is that swallowed glutathione gets broken down before much of it reaches circulation, so injecting it is meant to raise blood levels more reliably. Clinics use it off-label for skin brightening, general antioxidant support, and sometimes as an add-on in liver-related protocols, though the evidence behind most of those uses is still fairly thin.
Are glutathione injections actually safe, and what should someone worry about?
Safety here depends almost entirely on where the product came from and who is giving it. Compounded glutathione made under pharmacy sterility standards and given by a trained clinician carries a very different risk profile than a vial ordered from an unregulated website. The documented concerns with unverified sources include contamination, incorrect pH, and unlisted additives. Even properly sourced preparations can cause injection-site reactions and, occasionally, allergic responses. There’s no solid long-term safety data on repeated high-dose injections, and any provider worth trusting will say that upfront rather than gloss over it.
How much glutathione is used per injection, and who should be making that call?
Typical doses in clinical and aesthetic settings run from 600 mg to 1,200 mg per session, though that range comes more from practitioner convention than from controlled-trial evidence. A prescribing clinician should be the one setting the dose, based on weight, health history, and the actual goal. Self-dosing from a research-chemical vial with no oversight is where things tend to go wrong, since there’s no standardized concentration and no one accountable if the numbers don’t add up.
Where on the body do these injections go, and does that matter?
Most clinical glutathione injections are given intravenously, intramuscularly into the deltoid or gluteal muscle, or occasionally as a slow IV push. The site matters because IV delivery reaches peak blood levels fastest, which also means it carries the highest risk if anything is off with the preparation. Intramuscular injections work more slowly and are generally considered lower-risk for outpatient use. A physician-supervised compounding route, like the one FormBlends uses, specifies the intended route on the prescription itself, so the preparation is formulated correctly for that particular method.
References
- Witschi, A., et al. “The systemic availability of oral glutathione.” European Journal of Clinical Pharmacology, 1992. PMID 1362956
- Johnstone, C., et al. Case series on acute systemic inflammatory reactions following contaminated IV glutathione infusions. Epidemiology and Infection, 2018. PMID 29673413
- U.S. FDA. “FDA warns compounders not to use glutathione (Letco Medical) to compound sterile drugs.” fda.gov
- “Glutathione for skin lightening: a narrative review.” Cureus, 2025. PMC11862975
- Philippine FDA. “FDA Advisory No. 2019-182: Unsafe use of glutathione as skin lightening agent.” fda.gov.ph
Written by Sena Okafor, health correspondent. Last reviewed March 2026.
Nothing in this article is medical advice. Consult a licensed provider about your specific needs.
